We offer high-touch care coordination services to help individuals with the greatest medical and social vulnerability achieve sustainable, improved health outcomes.
Our care coordination team, comprised of social workers, registered nurses, and physicans, offers a social and medical lens to work with clients in identifying and addressing the root causes of poor health in a collaborative manner with other agencies.

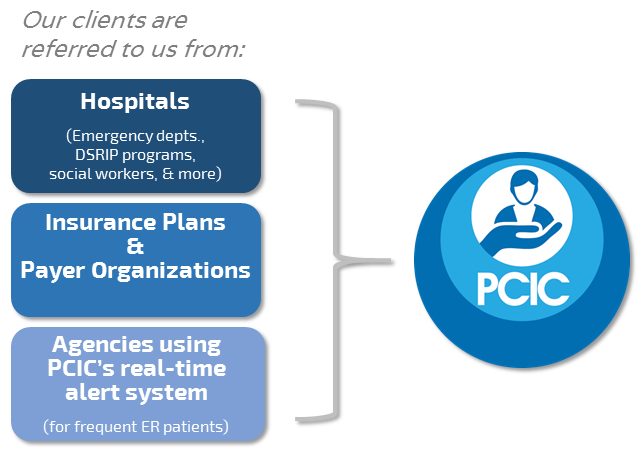
Who do we serve?
We serve clients with complex social and medical needs, many of whom are dual-eligible for Medicare and Medicaid.
Our clients are referred to us by hospitals and insurance plans, or through our internal automatic referral platform which tracks emergency service utilization across the Houston region and notifies us if an individual is visiting the emergency room at an unusually high rate.
How does our Care Coordination program work?
- Personalized health plan
- Connect to appropriate resources
- Track progress towards goals, service utilization, and changes in healthcare costs
Our team meets clients in the community or home each week for up to six months. We get to know clients, their values, and their health goals to develop a personalized health plan. We accompany clients on their doctor’s appointments to help them understand their diagnoses and develop next steps for improving their quality of life.
While serving clients, our care coordination team uses our internally developed comprehensive health management software to track clients’ progress towards accomplishing their health goals. The software has built-in dashboards to track healthcare costs and service utilization before, during, and after enrolling in our program.
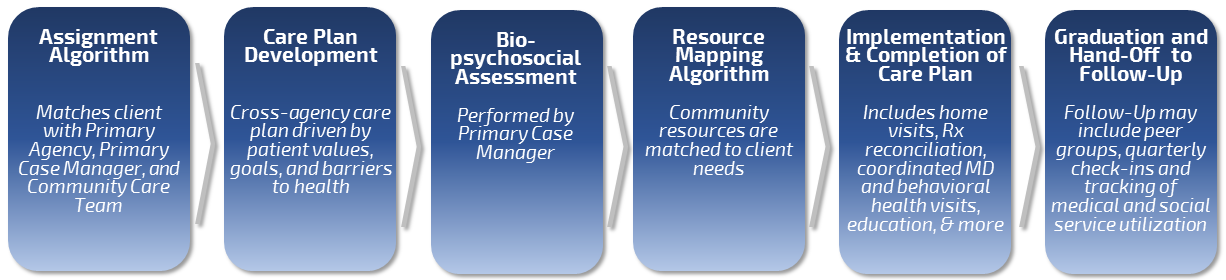
Once clients are enrolled in our program, the Care Coordination workflow is as follows:
Below are examples of what we’ve helped clients do in the past:
- Schedule appointments with the right doctors at the right time
- Contact insurance companies to help them gain access to resources, such as home health providers, home health nurses, assistive medical equipment, and more
- Coordinate transportation to get to medical appointments
- Get affordable medications
- Identify and coordinate housing opportunities if they are unstably housed or homeless
- Coordinate long-term care plans with family and primary care doctors to set up a plan for sustained health and wellbeing
What is the impact of our program?
After graduating from our care coordination program, our clients have a better understanding of their health needs, how to access appropriate resources to address those needs, and an increased sense of self-agency and trust of the medical system.
As a result, our graduated clients see on average a 37% decrease in hospital visits and a 20% improvement in quality of life measures (DLA-20), which leaves clients better able to live their lives as they want.
In doing so, we’ve saved the healthcare system (hospitals and insurance companies) over $9.2 Million and are scaling to achieve over $100M in savings over the next five years.
